The story of David Lander, aka Squiggy, started in Brooklyn, NY, in 1947. As a teenager, Lander attended the High School of Performing Arts in Manhattan and later attended college at NYU and Carnegie Tech.
After moving to Hollywood, Lander did some minor roles and was eventually discovered because of his unique voice and humor as he worked for an answering service. He was then given a job on a radio program called “The Credibility Gap”, a humorous news show.
It was at this radio station that David Lander met his future “Laverne and Shirley” sidekick Michael McKean, and the two put together the team of Lenny and Squiggy. One night, Penny Marshall just happened to be listening to their live show, and had the two audition for her father’s new sitcom “Laverne and Shirley”, in which she was starring. Soon Lenny and Squiggy were nationally known.
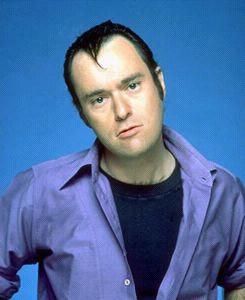
I remember watching this show as a kid and just howling over some of the crazy antics. My favorite scenes were when Lenny and Squiggy, the two deranged neighbors, would pop in. Squiggy (did you know that his full name was Andrew “Squiggy” Squiggmann?) always appeared to be some clown with a hair-brained plan that involved the girls. Too funny.
Not so funny is the fact that in real life, David Lander began to experience symptoms of multiple sclerosis shortly after the show ended (1985.) During this time period, there wasn’t a lot to do about modifying the disease— disease modifiers didn’t hit the market until the 1990’s— and Lander’s doctor told him he had a good chance of ending up in a wheelchair.
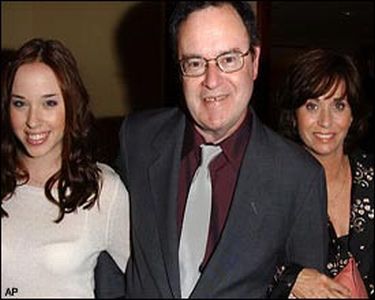
David consulted with his wife and daughter about what to do. It was decided that he would keep silent in order to protect his career, since aging and being sickly were (and are) highly frowned upon in Hollywood. He went on to do voiceovers for a number of feature films and TV shows, including “A Bug’s Life”, “Jungle Cubs”, and “101 Dalmatians.” Appearing in several other films, he was featured as the baseball game announcer in “A League of Their Own.”
Finally in 1999, Lander publically announced that he had MS. He was not in a wheelchair, but he admitted that he suffered from some of the embarrassing social blunders that multiple sclerosis can cause, such as unsteady walking and dropping things. In 2000, he was named the national MS Society Ambassador of the Year for his work at promoting MS awareness. In the same year Lander published his autobiography Fall Down Laughing: How Squiggy Caught Multiple Sclerosis and Didn’t Tell Nobody.
David Lander’s biggest piece of advice to anyone with MS is to fight it. He strongly advocates the use of any of the disease-modifying drugs and says that when he gives himself an injection, he thinks, “Wow! Look what I did for me.” He still works closely with the Nat’l MS society to promote MS awareness.
Probably the most unique thing about David Lander is his current baseball career: “I use to own a team in Portland. I owned 5 percent of the Portland Beavers, but now I’m a scout for the Seattle Mariners,” he says.
References:
